Therapists Working With Families or Groups Usually Practice Some Sort of _____ Therapy.
Gil, a 40-year-old Mexican American human, lives in an upper middle class neighborhood. He has been married for more 15 years to his high school sweetheart, a White American woman, and they have two children. Gil owns a armada of street-sweeping trucks—a business organization started by his father-in-police force that Gil has expanded considerably. Of tardily, Gil has been spending more time at piece of work. He has also been drinking more than usual and dabbling in illicit drugs. Equally his drinking has increased, tensions between Gil and his wife have escalated. From Gil's perspective and that of some family members and friends, Gil is just a hard-working guy who deserves to take a beer as a reward for a hard day'due south piece of work. Many people in his Mexican American customs exercise non consider Gil's low-level daily drinking a trouble, particularly because he drinks primarily at dwelling.
Recently, Gil had an accident while working on one of his trucks. The treating md identified booze abuse as one of several health problems and referred him to a substance abuse treatment center. Gil attended, but argued all the while that he was not a borracho (drunkard) and did not need treatment. He distrusted the counselors, stating that seeking assist from professionals for a mental disorder was something that only gabachos (Whites) did. Gil was proud of his chapters to "concord his liquor" and felt anger and hostility toward those who encouraged him to reduce his drinking. Gil's feelings and attitudes were valid; they stemmed from and were influenced past the Mexican American culture and community in which he had been raised from infancy. Gil dropped out of treatment. When his wife threatened to divorce him if he did non have immediate action to deal with his drinking problem, he reluctantly enrolled in an outpatient treatment program. Gil, like all people, is a product of his environment—an surroundings that has provided him with a rich cultural and spiritual background, a strong male identity, a deep zipper to family and community, a strong piece of work ethic, and a sense of pride in being able to back up his family. In many Mexican American cultural groups, illness disrupts family unit life, piece of work, and the ability to earn a living. Disease has psychological costs as well, including threats to a man'southward self-identity and sense of manhood (Sobralske 2006). Given this background, Gil would understandably be reluctant to enter treatment, to accept the fact that his drinking was a trouble or an illness, and to jeopardize his power to care for his family and his visitor. A culturally competent counselor would recognize, legitimize, and validate Gil's reluctance to enter and continue in treatment. In an ideal situation, the treatment counselor would have experience working with people with similar backgrounds and behavior, and the treatment programme would be structured to change Gil'southward behavior and attitudes in a manner that was in keeping with his culture and community. His initial handling might have succeeded if the counselor had been culturally competent and the handling program had been culturally responsive.
Like Gil, all clients enter treatment conveying behavior, attitudes, conflicts, and problems shaped past their cultural roots as well equally their present-day realities. As with Gil, many clients enter handling with some reluctance and denial. Inquiry shows that if clients such every bit Gil are greeted past a culturally competent advisor, they are more likely to respond positively to treatment (Damashek et al. 2012; Griner and Smith 2006; Kopelowicz et al. 2012; Whaley and Davis 2007). The presence of counselors of whatsoever race or gender who are culturally competent in responding to the needs and problems of their clients can greatly assist customer recovery. Gaining regard, respect, and trust from clients is crucial for successful counseling outcomes (Ackerman and Hilsenroth 2003; Sue and Sue 2003a).
Effective therapy is an ongoing procedure of building relational bridges that engender trust and confidence. Sensitivity to the client's cultural and personal perspectives, genuine empathy, warmth, humility, respect, and acceptance are the tenets of all sound therapy. This chapter expands on these concepts and provides a general overview of the core competencies needed so that counselors may provide effective treatment to diverse racial and ethnic groups. Using Sue'southward (2001) multidimensional model for developing cultural competence, the content focuses on the advisor'southward need to engage in and develop cultural awareness; cultural knowledge in general; and culturally specific skills and knowledge of wellness, mental disease, substance use, treatments, and skill development.
Core Counselor Competencies
Since Sue et al. introduced the phrase "multicultural counseling competencies" in 1992, researchers and academics accept elaborated on the core skill sets that enable counselors to work with diverse populations (American Psychological Association [APA] 2002; Council of National Psychological Associations for the Advancement of Ethnic Minority Interests 2009; Pack-Brown and Williams 2003; Tseng and Streltzer 2004). Cultural competence has evolved into more than a discrete skill set or knowledge base; it also requires ongoing self-evaluation on the office of the practitioner. Culturally competent counselors are aware of their ain cultural groups and of their values, assumptions, and biases regarding other cultural groups. Moreover, culturally competent counselors strive to understand how these factors affect their ability to provide culturally constructive services to clients.
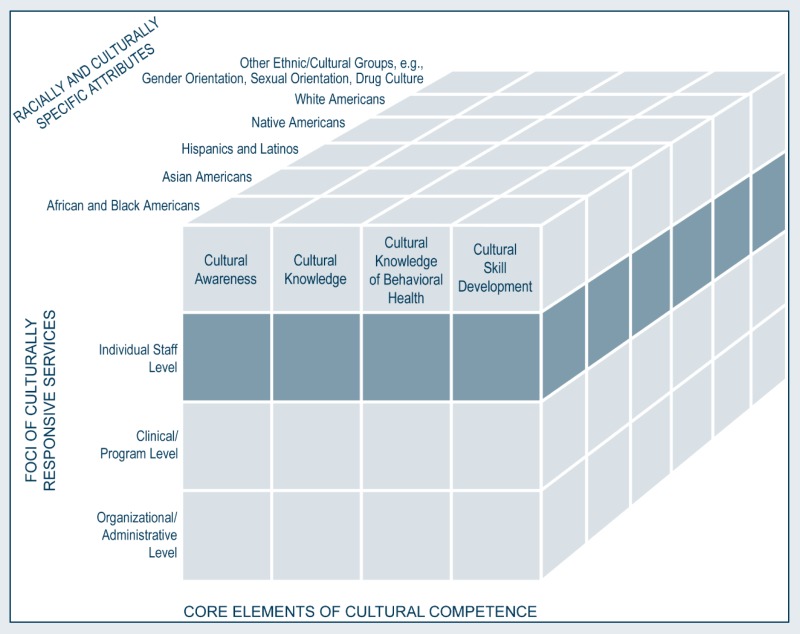
Multidimensional Model for Developing Cultural Competence: Individual Staff Level
Given the circuitous definition of culture and the fact that racially and ethnically various clients correspond a growing portion of the client population, the need to update and expand guidelines for cultural competence is increasing. The consensus panel thus adapted existing guidelines from the Clan of Multicultural Counseling for culturally responsive behavioral health services; some of their fundamental suggestions for counselors and other clinical staff are outlined in this affiliate.
Self-Knowledge
Counselors with a strong belief in evidence-based handling methods tin discover it difficult to relate to clients who prefer traditional healing methods. Conversely, counselors with strong trust in traditional healers and culturally accepted methods tin fail to empathize clients who seek scientific explanations of, and solutions to, their substance corruption and mental health issues. To get culturally competent, counselors should begin by exploring their ain cultural heritage and identifying how it shapes their perceptions of normality, abnormality, and the counseling process.
Counselors who sympathise themselves and their own cultural groups and perceptions are ameliorate equipped to respect clients with diverse belief systems. In gaining an awareness of their cultures, attitudes, beliefs, and assumptions through self-examination, training, and clinical supervision, counselors should consider the factors described in the following sections.
Cultural awareness
Counselors who are aware of their own cultural backgrounds are more likely to acknowledge and explore how culture affects their client–counselor relationships. Without cultural awareness, counselors may provide counseling that ignores or does not accost obvious issues that specifically chronicle to race, ethnic heritage, and civilisation. Lack of awareness can discount the importance of how counselors' cultural backgrounds—including beliefs, values, and attitudes—influence their initial and diagnostic impressions of clients. Without cultural awareness, counselors can unwittingly use their ain cultural experiences every bit a template to prejudge and assess client experiences and clinical presentations. They may struggle to run across the cultural uniqueness of each customer, assuming that they sympathize the customer'south life experiences and background better than they really do. With cultural awareness, counselors examine how their ain beliefs, experiences, and biases bear on their definitions of normal and abnormal behavior. By valuing this awareness, counselors are more probable to take the fourth dimension to sympathise the customer'southward cultural groups and their office in the therapeutic process, the client's relationships, and his or her substance-related and other presenting clinical problems. Cultural awareness is the first stride toward becoming a culturally competent advisor.
Racial, ethnic, and cultural identities
A key step in attaining cultural competence is for counselors to become aware of their own racial, ethnic, and cultural identities. Although the constructs of these identities are complex and difficult to define briefly, what follows is an overview. Racial identity "refers to a sense of group or collective identity based on one's perception that he or she shares a common heritage with a particular racial group" (Helms 1990, p. iii). Ethnic and cultural identity is "often the frame in which individuals place consciously or unconsciously with those with whom they experience a mutual bond because of like traditions, behaviors, values, and behavior" (Chavez and Guido-DiBrito 1999, p. 41). Culture includes, only is not limited to, spirituality and organized religion, rituals and rites of passage, language, dietary habits (east.g., attitudes toward food/food preparation, symbolism of food, religious taboos of food), and leisure activities (Bhugra and Becker 2005).
Models of Racial Identity
Models of racial identity, often structured in stages, highlight the process that individuals undertake in condign aware of their sense of self in relation to race and ethnicity within the context of their families, communities, societies, and cultural histories. Influenced past the Civil Rights Motion, earlier racial identity models in the United States focused on White and Black racial identity development (Cross 1995; Helms 1990; Helms and Carter 1991). Since so, models accept been created to incorporate other races, ethnicities, and cultures.
Although this affiliate highlights 2 formative racial identity models (see next page), additional resources highlight racial identity models that comprise other diverse groups, including those individuals who identify as multiracial (due east.g., come across Wijeyesinghe and Jackson 2012).
Aspects of racial, ethnic, and cultural identities are not ever apparent and do non always gene into conscious processes for the counselor or client, only these factors still play a role in the therapeutic human relationship. Identity evolution and formation help people make sense of themselves and the world around them. If positive racial, ethnic, and cultural messages are not bachelor or supported in behavioral health services, counselors and clients tin can lack affirmative views of their ain identities and may internalize negative messages or feel asunder from their racial and cultural heritages. Counselors from mainstream society are less likely to be actively aware of their own indigenous and cultural identities; in item, White Americans are not naturally drawn into examining their cultural identities, as they typically experience no dissonance when engaging in cultural activities.
In working to attain cultural competence, counselors must explore their own racial and cultural heritages and identities to gain a deeper agreement of personal development. Many models and theories of racial, indigenous, and cultural development are available; two mutual processes are presented below. Showroom 2-ane highlights the racial/cultural identity development (R/CID) model (Sue and Sue 1999b) and the White racial identity development (WRID) model (Sue 2001). Although before work focused on a linear developmental process using stages, current thought centers on a more flexible process whereby identification status can loop back to an earlier process or move to a later on stage.
Exhibit 2-i
Stages of Racial and Cultural Identity Development.
Using either model, counselors tin explore relational and clinical challenges associated with a given phase. Without an agreement of the cultural identity development process, counselors—regardless of race or ethnicity—can unwittingly minimize the importance of racial and indigenous experiences. They may fail to identify cultural needs and secure appropriate treatment services, unconsciously operate from a superior perspective (e.k., judging a specific beliefs every bit ineffectual, a sign of resistance, or a symptom of pathology), internalize a client'southward reaction (e.g., an African American advisor feeling betrayed or inadequate when a client of the aforementioned race requests a White American counselor for therapy during an initial interview), or view a client's behavior through a veil of societal biases or stereotypes. By acknowledging and endorsing the active process of racial and cultural identity development, counselors from diverse groups can normalize their own evolution processes and increase their sensation of clients' parallel processes of identity development. In counseling, racial, ethnic, and cultural identities can be pivotal to the handling procedure in the relationships not only between the counselor and customer, but among everyone involved in the delivery of the customer'southward behavioral health and chief care services (e.g., referral sources, family members, medical personnel, administrators). The instance study on page 41 uses stages from the two models in Exhibit 2-1 to bear witness the interactive process of racial and cultural identity development in the handling context.
Cultural and racial identities are non static factors that just mediate individual identity; they are dynamic, interactive developmental processes that influence one'south willingness to acknowledge the furnishings of race, ethnicity, and culture and to act against racism and disparity across relationships, situations, and environments (for a review of racial and cultural identity evolution, come across Sue and Sue 2013c). For counselors and clinical supervisors, it is essential to understand the dynamic nature of cultural identity in all exchanges. Starting with a personal appraisal, clinical staff members can begin to reflect—without judgment—on how their own racial and cultural identities influence their decisions, treatment planning, instance presentation, supervision, and interactions with other staff members. Clinicians can map the interactive influences of cultural identity development among clients, the clients' families, staff members, the organization, other agencies, and any other entities involved in the customer's handling. Using mapping (see the "How To Map Racial and Cultural Identity Development" box on the next folio) equally preparation for counseling, handling planning, or clinical supervision, clinicians tin can proceeds awareness of the many forces that influence culturally responsive treatment.
Example Study for Counselors: Racial and Cultural Identity
The client is a 20-yr-old Latino man. His male parent immigrated to the United states from Mexico every bit a child, and his female parent (of Latino/Middle Eastern descent) grew up about Albuquerque, New Mexico. Throughout the initial phase of mental wellness treatment, the client presented feelings, attitudes, and behavior consequent with the resistance and immersion stage of the R/CID model. During grouping counseling in a partial hospitalization program, the client said that he did non retrieve treatment was going to work. He believed that no one in treatment, except other Latino men, actually understood him or his life experiences. He idea that his low mood was due, in function, to his recent job loss.
The client's current concerns, symptoms, and diagnosis (bipolar I) were presented and discussed during the handling team meeting. The customer'south counselor (a White American man in the dissonance phase of the WRID model) was concerned that the client might leave treatment against medical advice and also stated that this would not exist the commencement time a Latino client had washed so. The team recognized that a Latino counselor would probable be useful in this situation (depending on the counselor's cultural competence). Nevertheless, no Latino counselor was available, and so the team decided that the client'due south current counselor should endeavour to proceeds support from the client's parents to encourage the customer to stay in treatment.
Considering the client had signed an appropriate release of information, his counselor was able to contact the parents and adapt a family session. During the family session, the advisor brought up the client's need for a Latino counselor. His parents disagreed, expressing their belief that it was important for their son to learn to chronicle to the counselor. They said that this was just an excuse their son was using to leave treatment, which had happened before. The parents' reaction exemplified a conformity response, although other data would need to take been gathered to make up one's mind their electric current stage more than accurately.
The counselor, client, parents, and system were operating from unlike stages of racial and cultural identity development. Because the lack of a proactive plan to provide appropriate resource—including the hiring of Latino staff or the development of other culturally appropriate resources (e.g., a peer counselor program)—the arrangement was nearly likely in the conformity phase of the WRID model. The counselor had some awareness of the client's racial and cultural needs and of the organization'south failure to meet them, just he alienated the client despite his good intentions and reinforced mistrust by engaging the client's parents before working straight with the client. Had the counselor taken the time to understand the client's concerns and needs, he would probable have created an opportunity to challenge his ain beliefs, larn more about the client's racial and cultural experiences and values, abet for more appropriate resource for the client inside the organization, be more flexible with handling solutions, and enable the client to have an experience that exceeded his expectations of the treatment provider.
Worldview: The cultural lens of counseling
The term "worldview" refers to a set of assumptions that guide how one sees, thinks about, experiences, and interprets the globe (Koltko-Rivera 2004). Starting in early childhood, worldview development is facilitated by significant relationships (particularly with parents and family members) and is shaped by the individual'due south environment and life experiences, influencing values, attitudes, beliefs, and behaviors. In more simplistic terms, each person's worldview is like a pair of glasses with colored lenses—the person takes in all of life's experiences through his or her own uniquely tinted view. Not unlike clients, counselors enter the treatment process with their own cultural worldviews that shape their concept of time; definition of family; organization of priorities and responsibilities; orientation to self, family, and/or community; religious or spiritual beliefs; ideas about success; and then on (Exhibit two-ii).

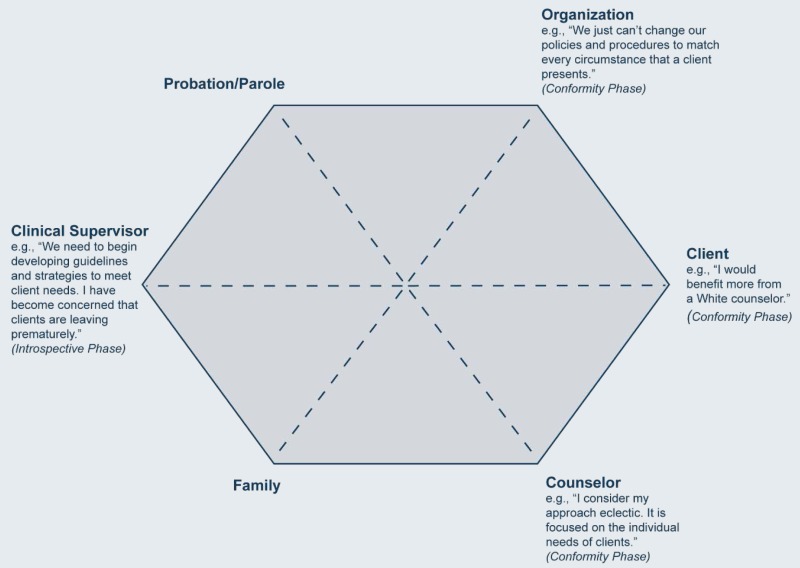
How To Map Racial and Cultural Identity Evolution
Completing this diagram can give a clearer perspective on past and anticipated dialog among key stakeholders. The diagram can be used as a training tool to teach racial and cultural identity development, to help clinicians and organizations recognize their own development, to explore clinical bug and dialogs that occur when diverse parties are at similar or unlike developmental stages, and to develop tools and resources to address issues that arise from this developmental process. Using instance studies, this diagram can serve as an interactive educational exercise to help counselors, clinical supervisors, and agencies gain awareness of the furnishings of race, ethnicity, and cultural groups.
Materials needed: Paper and pencils; handouts on the R/CID and WRID models.
Instructions
-
Identify all relevant parties, including client, advisor, family, supervisor, referral source, other staff members, and staff from other agencies (e.g., probation/parole, medical center/office, child and youth services). Include yourself. Place the names at each intersection of the hexagon.
-
List the common statements and behaviors (including lack of verbal responses) that you witness regarding the cultural needs of the client and/or the general statements made by each party regarding race, ethnicity, and culture. Write these every bit ane-line abbreviated phrases that represent each person/agency's opinion under the advisable entry on the diagram.
-
Using electric current information, choose the cultural identity development stage that best fits the statements or behaviors (knowing that you may be inaccurate); write it under each proper name.
However, counselors also debate with some other worldview that is often invisible but still powerful—the clinical worldview (Bhugra and Gupta 2010; Tilburt and Geller 2007; Tseng and Streltzer 2004). Influenced by educational activity, clinical grooming, and work experiences, counselors are introduced into a culture that reflects specific counseling theories, techniques, handling modalities, and full general part practices. This worldview, coupled with their personal cultural worldview, significantly shapes the counselor's beliefs pertaining to the nature of health, disease, and healing; interviewing skills and beliefs; diagnostic impressions; and prognosis. Moreover, it influences the definition of normal versus abnormal or disordered behavior, the determination of handling priorities, the ways of intervention, and the definitions of successful outcomes and treatment failures.
Foremost, counselors demand to remember that worldviews are often unspoken and inconspicuous; therefore, considerable reflection and self-exploration are needed to place how their own cultural worldviews influence their interactions both inside and outside of counseling. Clinical staff members demand to question how their perspectives are perpetuated in and shape client–counselor interactions, treatment decisions, planning, and selected counseling approaches. In sum, culturally responsive practice involves an understanding of multiple perspectives and how these worldviews interact throughout the treatment process—including the views of the counselor, client, family unit, other clients and staff members, treatment plan, organization, and other agencies, also as the community.
Stereotypes, prejudices, and history
Cultural competence involves counselors' willingness to explore their own histories of prejudice, cultural stereotyping, and discrimination. Counselors need to be aware of how their own perceptions of self and others have evolved through early babyhood influences and other life experiences. For instance, how were stereotypes of their own races and ethnic heritages perpetuated in their upbringing? What myths and stereotypes were projected onto other groups? What historical events shaped experiences, opportunities, and perceptions of self and others?
Regardless of their race, cultural group, or ethnic heritage, counselors need to examine how they accept directly or indirectly been affected by individual, organizational, and societal stereotypes, prejudice, and bigotry. How have certain attitudes, beliefs, and behaviors functioned as deterrents to obtaining equitable opportunities? In what ways have discrimination and societal biases provided benefits to them as individuals and as counselors? Even though these questions tin be uncomfortable, difficult, or painful to explore, sensation is essential regarding how these issues affect one'south function as a counselor, status in the organization, and comfort level in exploring clients' life experiences and perceptions during the treatment process. If counselors avoid or minimize the relevance of bias and bigotry in cocky-exploration, they volition probable do the aforementioned in the assessment and counseling process.
All counselors should examine their stereotypes, prejudices, and emotional reactions toward others, including individuals from their own races or cultural backgrounds and individuals from other groups. They should examine how these attitudes and biases may be detrimental to clients in handling for substance-related and mental disorders.
Clients tin can accept behavioral health issues and healthcare concerns associated with discrimination. If counselors are blind to these bug, they can miss vital information that influences client responses to treatment and willingness to follow through with continuing intendance and ancillary services. For example, a counselor may refer a client to a treatment plan without noting the client's history or perceptions of the recommended programme or type of program. The customer may initially agree to attend the program merely not follow through because of past negative experiences and/or the perception within his or her racial/ethnic community that the service does not provide adequate treatment for clients of colour.
Trust and power
Counselors need to understand the bear upon of their function and condition within the client–counselor relationship. Client perceptions of counselors' influence, power, and control vary in diverse cultural contexts. In some contexts, counselors tin can exist seen as all-knowing professionals, but in others, they tin be viewed as representatives of an unjust system. Counselors need to explore how these dynamics affect the counseling process with clients from various backgrounds. Exercise customer perceptions inhibit or facilitate the process? How do they touch the level of trust in the client–advisor human relationship? These issues should be identified and addressed early in the counseling process. Clients should take opportunities to talk about and process their perceptions, by experiences, and current needs.
Practicing within limits
A key element of ethical care is practicing within the limits of one'south competence. Counselors must engage in self-exploration, disquisitional thinking, and clinical supervision to empathise their clinical abilities and limitations regarding the services that they are able to provide, the populations that they can serve, and the treatment issues that they have sufficient training to accost. Cultural competence requires an ability to assess accurately one's clinical and cultural limitations, skills, and expertise. Counselors adventure providing services beyond their expertise if they lack awareness and noesis of the influence of cultural groups on client–advisor relationships, clinical presentation, and the treatment process or if they minimize, ignore, or avoid viewing treatment in a cultural context.
Communication to Counselors and Clinical Supervisors: Using the RESPECT Mnemonic To Reinforce Culturally Responsive Attitudes and Behaviors
-
Respect—Understand how respect is shown within given cultural groups. Counselors demonstrate this attitude through verbal and nonverbal communications.
-
Eastxplanatory model—Devote fourth dimension in treatment to agreement how clients perceive their presenting issues. What are their views about their ain substance abuse or mental symptoms? How practice they explain the origin of electric current bug? How similar or different is the advisor'south perspective?
-
Sociocultural context—Recognize how class, race, ethnicity, gender, didactics, socioeconomic status, sexual and gender orientation, immigrant condition, community, family, gender roles, and so forth affect intendance.
-
Power—Acknowledge the power differential betwixt clients and counselors.
-
Empathy—Express, verbally and nonverbally, the significance of each client's concerns and then that he or she feels understood by the counselor.
-
Concerns and fears—Elicit clients' concerns and apprehensions regarding help-seeking behavior and initiation of treatment.
-
Therapeutic alliance/Trust—Commit to behaviors that enhance the therapeutic relationship; recognize that trust is not inherent but must be earned by counselors.
Sources: Bigby and American Higher of Physicians 2003; Campinha-Bacote et al. 2005.
Some counselors may assume that they accept cultural competence based on having like experiences as clients, existence from the aforementioned race as clients, identifying every bit a member of the same ethnic heritage or cultural group as clients, or attention grooming on cultural competence. Other counselors may assume competence based on their current or prior relationships with others from the same race or cultural background equally their clients. These experiences tin can be helpful and filled with many potential learning opportunities, but they do not brand an individual eligible or competent to provide multicultural counseling. Too, the assumption that a person from the same cultural group, race, or ethnic heritage will intrinsically understand a customer from a similar background is operating out of ii common myths: the "myth of sameness" (i.eastward., that people from the same cultural group, race, or ethnicity are alike) and the myth that "familiarity equals competence" (Srivastava 2007). The Association for Multicultural Counseling and Development adopted a fix of advisor competencies that was endorsed by the American Counseling Association (ACA) for counselors who work with a multicultural clientele (Showroom 2-3). Competencies address the attitudes, behavior, cognition, and skills associated with the counselor's need for self-knowledge.
![]()
Showroom 2-iii
ACA Advisor Competencies: Counselors' Sensation of Their Own Cultural Values and Biases.
Cognition of Other Cultural Groups
In addition to an understanding of themselves and how their cultural groups and values can bear upon the therapeutic process, culturally competent counselors work to learn cultural knowledge and agreement of clients and staff with whom they work. From the outset, counselors need general cognition and awareness when working with other cultural groups in counseling. For case, they should acknowledge that culture influences advice patterns, values, gender roles and socialization, clinical presentations of distress, counseling expectations, and behavioral norms and expectations in and exterior the counseling session (e.g. , touching, greetings, souvenir-giving, accessory in sessions, level of formality between counselor and client). Counselors should filter and interpret client presentation from a broad cultural perspective instead of using just their own cultural groups or previous client experiences as reference points.
Counselors also need to invest the time to know clients and their cultures. Culturally responsive practise involves a commitment to obtaining specific cultural knowledge, non but through ongoing client interactions, but as well through the use of outside resources, cultural training seminars and programs, cultural events, professional consultations, cultural guides, and clinical supervision. Counselors need to be mindful that they will not know everything nigh a specific population or initially comprehend how an private customer endorses or engages in specific cultural practices, behavior, and values. For instance, some clients may non identify with the same cultural behavior, practices, or experiences as other clients from the aforementioned cultural groups. Still, counselors demand to be as knowledgeable equally possible and attend to these cultural attributes—start with the intake and cess process and continuing throughout the counseling and handling human relationship. For a review of content areas essential in knowing other cultural groups, refer to the "What Are the Cross-Cutting Factors in Race, Ethnicity, and Civilization" department in Chapter 1. These cultural knowledge content areas include:
-
Geographic location.
-
Worldview, values, and traditions.
-
Family and kinship.
-
Gender roles.
-
Socioeconomic status and education.
-
Heritage and history.
-
Sexuality.
-
Religion and spirituality.
-
Health, disease, and healing.
"Become familiar with the community in which the client lives and the general cultural norms of the individual client. This tin can be accomplished by visiting with people who know the customs well, attending important community celebrations and other events, request open-ended questions almost community concerns and quality of life, and identifying community capacities that affect wellness in the customs."
(Perez and Luquis 2008, p. 177)
Counselors should not make assumptions most clients' race, indigenous heritage, or culture based on appearance, accents, beliefs, or language. Instead, counselors need to explore with clients their cultural identity, which can involve multiple identities (Lynch and Hanson 2011). Counselors should discuss what cultural identity means to clients and how it influences treatment. For case, a immature developed two-spirited (gay) American Indian man may be more than concerned with having access to traditional healing practices than to specialized services for gay men. Counselors and clients should collaboratively examine presenting treatment issues and obstacles to engaging in behavioral health treatment and maintaining recovery, and they should hash out how cultural groups and cultural identities can serve as guideposts in treatment planning.
Showroom 2-four lists ACA-endorsed counselor competencies for knowledge of the worldviews of clients from diverse cultural groups.
![]()
Exhibit 2-4
ACA Counselor Competencies: Awareness of Clients' Worldviews.
Cultural Knowledge of Behavioral Wellness
Counselors should learn how culture interacts with health beliefs, substance use, and other behavioral wellness issues. They tin can access literature and grooming that address cultural contexts and meanings of substance apply, behavioral and emotional reactions, help-seeking behavior, and treatment. Chapter 5 gives data on culturally responsive behavioral wellness services for major ethnic and racial groups. The how-to box beneath lists means to improve one'due south cultural knowledge of health issues by acquiring knowledge in fundamental areas to piece of work successfully with various clients:
-
Patterns of substance use and handling-seeking behavior specific to people of diverse racial and cultural backgrounds.
-
Beliefs and traditions surrounding substance use, including cultural norms apropos the employ of alcohol and drugs.
-
Beliefs about treatment, including expectations and attitudes toward health intendance and counseling.
-
Customs perceptions of behavioral health treatment.
-
Obstacles encountered by specific populations that make it difficult to access treatment, such as geographic distance from handling services.
-
Patterns of co-occurring disorders and conditions specific to people from diverse racial and cultural backgrounds (e.one thousand., culturally specific syndromes, earlier onset of diabetes, college prevalence of low and substance dependence).
-
Assessment and diagnosis, including culturally appropriate screening and cess and awareness of mutual diagnostic biases associated with symptom presentation.
-
Private, family, and group therapy approaches that agree promise in addressing mental and substance-related disorders specific to the racial and cultural backgrounds of diverse clients.
-
Culturally appropriate peer support, mutual-assistance, and other support groups (eastward.g., the Wellbriety movement, a culturally appropriate 12-Step plan for Native American people).
-
Traditional healing and complementary methods (e.g., employ of spiritual leaders, herbs, and rituals).
-
Continuing care and relapse prevention, including attention to clients' cultural environments, treatment needs, and accessibility of care inside their communities.
-
Handling engagement/retention patterns.
How To Meliorate Cultural Knowledge of Health, Illness, and Healing
To promote culturally responsive services, counselors demand to acquire cultural cognition regarding concepts of health, illness, and healing. The post-obit questions highlight many of the culturally related bug that are prevalent in and pertinent to cess, treatment planning, and case management. This list of considerations can help facilitate discussions in counseling and clinical supervision contexts:
-
Does the cultural group in question consider psychological, physical, and spiritual health or well-beingness equally carve up entities or equally unified aspects of the whole person?
-
How are illnesses and healing practices divers and conceptualized?
-
What are acceptable behaviors for managing stress?
-
How exercise people who belong to the civilisation in question typically express emotions and emotional distress?
-
What behaviors, practices, or customs do members of this culture consider to be preventive?
-
What words do people from this cultural grouping use to describe a particular trouble?
-
How do members of the group explain the origins or causes of a particular condition?
-
Are there culturally specific weather or cultural concepts of distress?
-
Are there specific biological and physiological variations amidst members of this population?
-
What are the common symptoms that lead to misdiagnosis inside this population?
-
Where do people from this cultural group typically seek help?
-
What traditional healing practices and treatments are endorsed by members of this group?
-
Are there biomedical treatments or procedures that would typically be unacceptable?
-
Are at that place specific counseling approaches more coinciding with the beliefs of most members?
-
What are common health inequities, including social determinants of wellness, for this population?
-
What are acceptable caregiving practices?
-
Exercise members of this grouping attach award to caring for family members with specific diseases?
-
Are individuals with specific weather shunned from the community?
-
What are the roles of family members in providing wellness care and in making decisions?
-
Is discussing consequences of and prognosis for behaviors, atmospheric condition, or diseases acceptable?
-
Is it customary for family unit members to withhold prognosis from the client?
Skill Evolution
Becoming culturally competent is an ongoing procedure—ane that requires introspection, sensation, noesis, and skill development. Counselors need to develop a positive attitude toward learning about multiple cultural groups; in essence, counselors should commit to cultural competence and the process of growth. This commitment is evidenced via investment in ongoing learning and the pursuit of culturally coinciding skills. Counselors can demonstrate commitment to cultural competence through the attitudes and corresponding behaviors indicated in Showroom 2-5.
Showroom 2-5
Attitudes and Behaviors of Culturally Competent Counselors.
Beyond the commitment to and development of these cardinal attitudes and behaviors, counselors need to piece of work toward intervention strategies that integrate the skills discussed in the following sections.
Frame problems in culturally relevant ways
Counselors should frame clinical problems with culturally appropriate references. For case, in cultural groups that value the community or family as much every bit the individual, it is helpful to address substance abuse in light of its consequences to family unit or the community. The counselor might ask, "How are your family and community affected by your use? How practice family and community members feel when they see you high?" For clients who place more value on their independence, it can be more effective to point out how substance dependence undermines their power to manage their own lives through questions similar "How might your use touch your power to reach your goals?"
Allow for complication of bug based on cultural context
Counselors must take intendance with suggesting elementary solutions to complex problems. It is often better to admit the intricacies of the customer's cultural context and circumstances. For instance, a Native American single female parent who upholds traditional values could balk at a suggestion to stop spending fourth dimension with family members who drink heavily. Here, the counselor might encourage the woman to broaden support inside her community by connecting with an elder who supports recovery or by engaging in a women's talking circle. Likewise, a referral for a psychiatric evaluation for major depression may not be an appropriate initial recommendation for a Chinese customer who relies on cultural remedies and healing traditions. An culling approach would exist to explore the customer'due south beliefs in healing, develop steps that respect and incorporate the customer'southward help-seeking practices, and coordinate services to secure a culturally responsive intervention (Cardemil et al. 2011; Gallardo et al. 2012; Lynch and Hanson 2011).
Make allowances for variations in the use of personal space
Cultural groups have different expectations and norms of propriety concerning how close people can be while they communicate and how personal communications can exist depending on the type of relationship (e.grand., peers versus elders). The concept of personal space involves more than the concrete distance between people. It also involves cultural expectations regarding posture or stance and the employ of infinite within a given environment. These cultural expectations, although they are subtle, tin can have an impact on treatment. For case, an Alaska Native may feel more comfy sitting abreast a counselor, whereas a European may adopt to be separated from a advisor by a desk (Sue and Sue 2013a). The use of infinite tin can also be a nonverbal expression of power. Standing also shut to someone can, for example, advise power over them. Standing likewise far away or sitting behind a desk-bound can indicate apathy. Adequate or expected degrees of closeness betwixt people are culturally specific; counselors should exist educated on the general parameters and expectations of the given population. Nonetheless, counselors should not predetermine the clients' expectations; instead, they should follow the clients' lead and inquire well-nigh their preferences.
Advice to Counselors and Clinical Supervisors: Behaviors for Counselors To Avoid
-
Addressing clients informally; counselors should not assume familiarity until they grasp cultural expectations and client preferences.
-
Declining to monitor and adjust to the client's verbal pacing (e.g., not assuasive time for clients to respond to questions).
-
Using counseling jargon and handling language (eastward.m., "I am going to ship you to our principal stabilization programme to obtain a biopsychosocial and so, afterward, to partial").
-
Using statements based on stereotypes or other preconceived ideas generated from experiences with other clients from the same culture.
-
Using gestures without agreement their pregnant and appropriate context inside the given civilisation.
-
Ignoring the relevance of cultural identity in the client-counselor relationship.
-
Neglecting the client's history (i.east., not agreement the customer's individual and cultural background).
-
Providing an explanation of how electric current difficulties tin be resolved without including the customer in the process to obtain his or her own explanations of the issues and how he or she thinks these issues should be addressed.
-
Downplaying the importance of traditional practices and failing to coordinate these services equally needed.
Sources: Fontes 2008; Lynch and Hanson 2011; Pack-Brown and Williams 2003; Srivastava 2007.
Display sensitivity to culturally specific meanings of touch
Some treatment and many support groups take opening or closing traditions that include property hands or giving hugs. This course of touching can be very uncomfortable to new clients regardless of cultural groups; cultural prescriptions, including religious beliefs, concerning appropriate touching can compound this effect (Comas-Diaz 2012). Many cultural groups use touch to admit or greet someone, to show respect or convey status or power, or to display comfort. As counselors, it is essential to understand cultural norms nigh touch, which often are guided by gender and age, and the contexts surrounding "appropriate" bear upon for specific cultural groups (Srivastava 2007). Counselors need to devote time to agreement their clients' norms for and interpretations of bear on, to assisting clients in negotiating and upholding their cultural norms, and to helping clients sympathize the context and cultural norms that are likely to prevail in support and treatment groups.
Explore culturally based experiences of power and powerlessness
Ideas about ability and powerlessness are influenced past the client's culture and social form. What constitutes power and powerlessness varies from culture to culture according to the individual's gender, age, occupation, ancestry, religious affiliation, and a host of other factors. For example, power tin exist divers in terms of one's place within the family, with the oldest fellow member being the most powerful and the youngest being the least powerful. Even the words "ability" and "powerlessness" carry cultural pregnant. These words tin can acquit negative connotations for clients with histories of discrimination and multiple experiences with racism, for some women, for indigenous peoples with histories of colonization, and for refugees or immigrants who take left oppressive regimes. In this regard, counselors should use these words carefully. For example, a Hmong refugee who experienced trauma in her country of origin could already feel helpless and powerless over the events that occurred; thus, the concept of powerlessness, oft used in drug and alcohol handling programs, can exist contraindicated in addressing her substance-related disorder. Yet, a White American concern executive who has authority over others and a history of financial influence may need assist acknowledging that he cannot control his substance corruption.
Adjust advice styles to the client's culture
Cultural groups all have dissimilar communication styles. Norms for communicating vary in and between cultural groups based on form, gender, geographic origins, religion, subcultures, and other individual variations. Counselors should educate themselves as much every bit possible regarding the patterns of communicating in the client'southward cultural, racial, or indigenous population while also being aware of his/her own advice style. For a comprehensive guide in self-cess and understanding of communication styles, refer to Civilization Matters: The Peace Corps Cross-Cultural Workbook (Peace Corps Information Collection and Commutation 2012).
The following are general guidelines for ascertaining the client's communication manner:
-
Understand the customer's verbal and nonverbal ways of communicating. Be enlightened of the possible demand to move abroad from comprehending and interpreting customer responses in conventional professional ways (Bland and Kraft 1998). Always be curious well-nigh the client's cultural context and be willing to seek clarification and better understanding from the customer. Information technology is every bit important for counselors to access and appoint in cultural consultation to acquire more than specific noesis and experience.
-
Styles of communication and nonverbal methods of communication are important aspects of cultural groups. Issues such equally the advisable space to take between people; preferred means of moving, sitting, and standing; the pregnant of gestures; and the degree of center contact expected are all culturally defined and situation specific (Hall 1976). As an example, high-context cultural groups place greater importance on nonverbal cues and message context, whereas low-context cultural groups rely largely on exact bulletin content. Most Asian Americans come up from high-context cultural groups in which sensitive messages are encoded carefully to avoid offending others. A provider who listens only to the content could miss the bulletin. What is not said can possibly exist more than important than what is said.
-
Heed to storytelling carefully, every bit it can be a manner of communicating with the therapist. As in any skilful therapy, follow the associations and mind for possible metaphors to meliorate sympathize relational pregnant, cognition, and emotion within the context of the chat.
How To Appraise Differences in Advice Styles
This practice can be used by counselors and clinical supervisors equally a self-assessment tool and a ways of exploring differences in communication styles amongst counselors, clients, and supervisors. It can likewise serve as a group exercise to help clients talk over and understand cultural differences in communicating with others. This cocky-administered tool promotes self-understanding and cultural knowledge. It is not an empirically based instrument, nor is information technology meant to assess client communication styles or skills formally.
Materials needed: Colored pencils/pens and copies of the exercise.
Instructions
-
First, place an Ten along the line for each item that all-time matches your style or design of communication overall. Advice patterns can alter across situations and environments depending on expectations, stress level, and familiarity, (e.yard., attending a staff meeting versus spending time with friends); try to assign the fashion that best reflects your patterns beyond situations.
-
After reviewing your own patterns, compare differences between you and your customer, clinical supervisor, or young man staff member. For example, select a recent client you treated and place a second Ten (using a unlike color pen) on each line to mark your perceived view of this client's advice style. Then examine the differences betwixt you and your client and generate a listing of potential misunderstandings that could occur due to these differences. Use clinical supervision to hash out how your own patterns tin can hinder and/or promote the counseling process.
View in own window
| NONVERBAL PATTERNS | ||
|---|---|---|
| Heart Contact | ||
| When talking: Directly, sustained | | Indirect or not sustained |
| When listening: Straight, sustained | | Indirect or not sustained |
| Vocal Pitch/Tone | ||
| Loftier/loud | | Low/soft |
| More expressive | | Less expressive |
| Speech Charge per unit | ||
| Fast | | Slow |
| Pauses or Silence | ||
| Little use of silence in dialog | | Pauses; uses silence in dialog |
| Facial Expressions | ||
| Frequent expression | | Niggling expression |
| Use of Other Gestures | ||
| Frequent expression | | Petty expression |
| Exact PATTERNS | ||
| Emotional Expression | ||
| Does express and place feelings in oral communication | | Does non express or identify feelings in speech |
| Self-Disclosure | ||
| Frequently | | Rarely or petty |
| Formality | ||
| Informal | | Formal in addressing others and showing respect |
| Directness | ||
| Verbally explicit | | Indirect; subtle; doesn't believe in proverb everything |
| Context | ||
| Depression context; relies more on words to convey meaning | | High context: verbal and nonverbal cues convey much of the pregnant |
| Orientation | ||
| Orientation to cocky; utilize of "I" statements | | Orientation to others, use of plural and 3rd-person pronouns (east.one thousand., nosotros, he) |

Other Things To Consider in Exploring Advice Styles
-
Are there known differences in body language and expression within the given cultural group?
-
What are the mutual, culturally appropriate parameters of touch across situations? For case, a handshake could be advisable equally a ways of introduction for 1 cultural group but not for another.
-
How is personal space used in and exterior of the function? Are there known cultural patterns in the employ of space and proximity of communication?
-
What verbal and nonverbal advisor behaviors may impact trust in the counseling process?
Sources: Cormier et al. 2009; Fontes 2008; Srivastava 2007; Sue and Sue 2013a.
Translate emotional expressions in calorie-free of the client'south civilisation
Feelings are expressed differently across and within cultural groups and are influenced by the nature of a given event and the individuals involved in the state of affairs. A certain level of emotional expression tin be socially appropriate within i civilisation yet inappropriate in another. In some cultural groups, feelings may not exist expressed straight, whereas in other cultural groups, some emotions are readily expressed and others suppressed. For example, expressions of sadness may at first be more readily shared by some clients in counseling settings, whereas others may find information technology more comfortable to express anger as their initial response. Counselors must recognize that not all cultures identify the same value on verbalizing feelings. In fact, clients from some cultures may not perceive that emotional expression is a worthy grade of handling and healing at all. Thus, counselors should not impose a prescribed arroyo that measures progress and equates healing with the power to display emotions. Also, counselors should be conscientious not to aspect meaning based on their ain cultural backgrounds or to project their own feelings onto clients' experiences. Instead, counselors need to assist their clients in identifying and labeling feelings within their ain cultural contexts.
Aggrandize roles and practices
Counselors need to learn a mindset that allows for more flexible roles and practices—while nonetheless maintaining appropriate professional person boundaries—when working with clients. Some clients whose culture places considerable accent upon and orientation toward family could look to counselors for advice with unrelated issues pertaining to other family unit members. Other clients may expect a more than prescribed and structured approach in which counselors give specific recommendations and communication in the session. For instance, Asian American clients appear to expect and benefit from a more directive and highly structured approach (Fowler et al. 2011; Lee and Mock 2005a; Sue 2001; Uba 1994). Still others could expect that counselors be continued to their communities through participation in community events, in working with traditional healers, or in edifice collaborative relationships with other community agencies. As counselors, it is of import to understand the cultural contexts of clients and how this translates to expectations in the client–counselor human relationship. The appropriate role unremarkably Results from the advisor'due south agreement of and sensitivity to the values, cultures, and special needs of the individuals and groups being served (Sue and Sue 2013d). Counselors demand to prefer an ongoing commitment to developing skills and endorsing practices that assist clients in receiving and experiencing the best possible intendance. Exhibit ii-6 lists advisor competencies endorsed by ACA for culturally appropriate intervention strategies.
![]()
Exhibit 2-six
ACA Counselor Competencies: Culturally Advisable Intervention Strategies.
Providing good care goes across counselors' general knowledge, clinical skills, and approaches; it involves understanding the multicultural context of clients and of themselves every bit counselors. Cultural competence is an ethical upshot requiring counselors to be invested in developing the tools to provide culturally congruent care—care that matches the needs and context of the client. For a review of ethics and ethical dilemmas in a multicultural context, refer to Pack-Brown and Williams (2003).
Self-Assessment for Individual Cultural Competence
Several instruments for evaluating an private's cultural competence have been adult and are available online. One cess tool that has been widely circulated is Goode's Self-Assessment Checklist for Personnel Providing Services and Supports to Children and Youth With Special Health Needs and Their Families. It can be adapted for counselors treating adult clients with behavioral health concerns. This tool and other additional resources are provided in Appendix C. For an interactive Web-based tool on cultural competence awareness, visit the American Voice communication-Language-Hearing Association Spider web site (http://www.asha.org).
honeycutttherharded.blogspot.com
Source: https://www.ncbi.nlm.nih.gov/books/NBK248422/
0 Response to "Therapists Working With Families or Groups Usually Practice Some Sort of _____ Therapy."
Post a Comment